MICHELLE FERDERBAR 1217500
The exposure index (EI) value provided to the x-ray technologist is quite important when it comes to determining if the exposure factors used were appropriate for an image. In fact, that is exactly what EI values do - they let the technologist know that a digital image has been taken at appropriate technical factors to result in a good quality image. When film was more popular, it was much more obvious to the user that their image was over or underexposed because the image would appear too dark or too light, respectively. However, with the dawn of postprocessing in today's digital environments, it is well hidden. The EI value is the sole indicator to the technologist if their exposure was within an acceptable range because "neither the brightness nor the contrast of the image can be attributed entirely to the original radiographic technique" in digital imaging (Carroll, 2007). This lab was conducted in x-ray room 5, B114 of the Institute of Applied Health Sciences on the McMaster University Campus.
 Figure 1. Initial Set-up with dosimeter. | 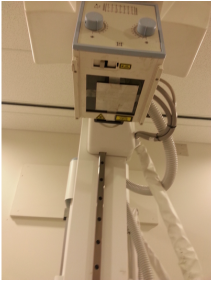 Figure 2. Aluminum Filter taped. | 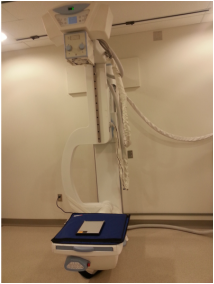 Figure 3. Cassette replaced the dosimeter. |
The procedure was fairly simple and is easy to incorporate into any quality control routine. To begin, we covered the detector with two lead aprons and placed the dosimeter onto this, as seen in Figure 1. We then adjusted the tube to have an SID of 172 cm. We collimated to the dosimeter's sensor. We then taped two sheets of 1 mm Al to the underside of the collimator, as seen in Figure 2. This means it is important to properly center before doing this step since you can no longer see the collimator light. We then set the technique to 80 kV and we adjusted the techniques to achieve a reading close to 10 mR. The attempts are summarized in Table 1. We found that at 8 mAs and an SID of 72 inches we were able to achieve a reading of 9.98 mR. We did it twice more to ensure we got the same result again.
At this point, we were able to continue. As seen in Figure 3, we then removed the aluminum and replaced the dosimeter with a 10 x 12 CR cassette then replaced the aluminum once ensuring that the light (still collimated from the dosimeter) was on the cassette. We adjusted to ensure an SID of 72 inches. We then exposed this and processed the cassette with the "Pattern" setting. This was repeated for two more cassettes.
At this point, we were able to continue. As seen in Figure 3, we then removed the aluminum and replaced the dosimeter with a 10 x 12 CR cassette then replaced the aluminum once ensuring that the light (still collimated from the dosimeter) was on the cassette. We adjusted to ensure an SID of 72 inches. We then exposed this and processed the cassette with the "Pattern" setting. This was repeated for two more cassettes.
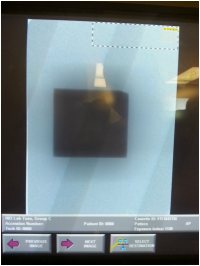 Figure 4. Image with EI value of 1130. | 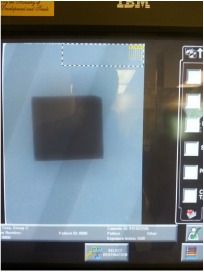 Figure 5. Image with EI value of 1420. |  Figure 6. Image with EI value of 1020. |
Figures 4, 5, and 6 demonstrate the processed images. The EI values were 1130, 1420, and 1020 respectively. The average value was calculated to be 1190. Before we discuss this further, it is pertinent to understand the system's EI value settings.
Kodak, now known as Carestream, calculated the EI value by 1000 x log(exposure in mR) + 2000. In this system, the desired ideal EI value range is 1800 - 2200 and any change of 300 is an indication of changing the exposure by a factor of 2. It is a logarithmic and directly proportional scale. At a reading of 2000 EI, 1 mR of exposure was received at the aforementioned settings. All of this can be read about in the PDF below (Gallet, 2010).
Kodak, now known as Carestream, calculated the EI value by 1000 x log(exposure in mR) + 2000. In this system, the desired ideal EI value range is 1800 - 2200 and any change of 300 is an indication of changing the exposure by a factor of 2. It is a logarithmic and directly proportional scale. At a reading of 2000 EI, 1 mR of exposure was received at the aforementioned settings. All of this can be read about in the PDF below (Gallet, 2010).
According to Samei et al. (2001), once normalized, a value of 2000 ± 45 is acceptable.
1130 - (1000 x log(9.98)) = 130.87 mR
1420 - (1000 x log(9.98)) = 420.87 mR
1020 - (1000 x log(9.98)) = 20.87 mR
Unfortunately, none of ours fit this criteria as they are all too low. Therefore, the system fails and is improperly calibrated.
There are consequences to an improperly calibrated CR processor. One of these consequences is that the technologist would get inaccurate readings about dosage to the patient. If a technologist kept getting overly low readings, such as in our case, the technologist may be inclined to increase the technique unnecessarily resulting in overexposing future patients. This could also result in strain on the x-ray machine due to the higher techniques. Another issue is that if the readings given were constantly too high, we would result in underexposed images, more dose to the patient, and highly mottled images. Since the goal of EI values are to inform the technologist if they are within proper dose ranges, losing that is the main consequence.
1130 - (1000 x log(9.98)) = 130.87 mR
1420 - (1000 x log(9.98)) = 420.87 mR
1020 - (1000 x log(9.98)) = 20.87 mR
Unfortunately, none of ours fit this criteria as they are all too low. Therefore, the system fails and is improperly calibrated.
There are consequences to an improperly calibrated CR processor. One of these consequences is that the technologist would get inaccurate readings about dosage to the patient. If a technologist kept getting overly low readings, such as in our case, the technologist may be inclined to increase the technique unnecessarily resulting in overexposing future patients. This could also result in strain on the x-ray machine due to the higher techniques. Another issue is that if the readings given were constantly too high, we would result in underexposed images, more dose to the patient, and highly mottled images. Since the goal of EI values are to inform the technologist if they are within proper dose ranges, losing that is the main consequence.
References
Gallet, J. (2010). Technical Brief Series: The Concept of Exposure Index for Carestream
Directview Systems. Retrieved from www.carestream.ca/cr-exposure-whitePaper-M1-461.pdf.
Health Canada. (2008). Safety code 35: Safety procedures for the installation, use and
control of x-ray equipment in large medical radiological facilities.
Retrieved from http://www.hc-sc.gc.ca.
Samei, E., Seibert, J., Willis, C., Flynn, M., Mah, E., & Junck, K. (2001). Performance Evaluation Of
Computed Radiography Systems. Medical Physics, 28(3), 361-371. DOI: 10.1118/1.1350586.
Service Ontario. (2011). Healing Arts Radiation Protection Act.
Retrieved from http://www.e-laws.gov.on.ca/html/regs/english/elaws_regs_900543_e.htm.
Carroll, Q. (2007). Practical Radiographic Imaging (8th ed.). Springfield: Charles C Thomas Publisher.
Directview Systems. Retrieved from www.carestream.ca/cr-exposure-whitePaper-M1-461.pdf.
Health Canada. (2008). Safety code 35: Safety procedures for the installation, use and
control of x-ray equipment in large medical radiological facilities.
Retrieved from http://www.hc-sc.gc.ca.
Samei, E., Seibert, J., Willis, C., Flynn, M., Mah, E., & Junck, K. (2001). Performance Evaluation Of
Computed Radiography Systems. Medical Physics, 28(3), 361-371. DOI: 10.1118/1.1350586.
Service Ontario. (2011). Healing Arts Radiation Protection Act.
Retrieved from http://www.e-laws.gov.on.ca/html/regs/english/elaws_regs_900543_e.htm.
Carroll, Q. (2007). Practical Radiographic Imaging (8th ed.). Springfield: Charles C Thomas Publisher.

 RSS Feed
RSS Feed
